Post cycle therapy is the phase people plan the least and regret skipping the most. You spent weeks planning your cycle, dialling your diet, tracking your lifts. Then the cycle ends and the plan stops. That is the most expensive mistake you can make, not in money, but in what happens to your hormones, your physique, and your health when your body is left to figure things out on its own.
This guide covers what PCT actually is, what happens if you skip it, the three main drugs used and how they differ, exactly when to start based on what you ran, how long to run it, and whether SARMs need it too.
What Is Post Cycle Therapy?
Post cycle therapy (PCT) is a structured protocol used after a cycle of anabolic steroids, SARMs, or other performance-enhancing compounds to restart the body’s natural testosterone production.
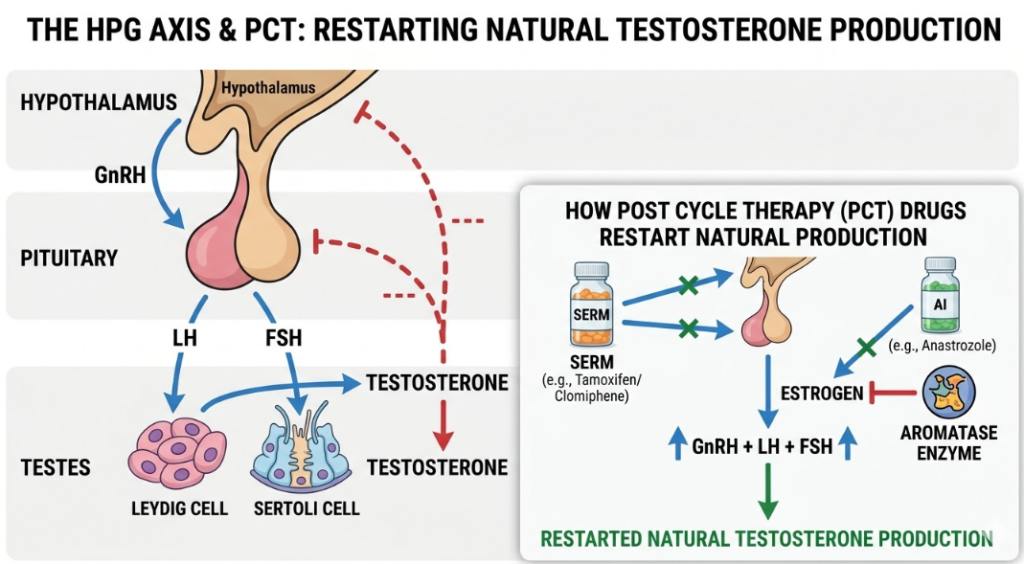
During any steroid cycle, your body detects elevated androgen levels and shuts down its own hormone signalling. The hypothalamic-pituitary-gonadal (HPG) axis goes quiet: the brain stops releasing GnRH, the pituitary stops releasing LH and FSH, and the testes stop producing testosterone. When the cycle ends, that shutdown does not automatically reverse.
PCT uses specific medications, primarily SERMs and sometimes hCG, to stimulate that signalling chain back into action, restoring natural testosterone production faster than your body would manage alone.
What Happens If You Skip PCT?
This is where most guides get vague. Here is what actually happens in the weeks after a cycle ends without PCT.
Testosterone crashes. Oestrogen does not, it often rebounds as the testosterone-to-oestrogen ratio swings wildly. The result is a catabolic hormonal environment where your body begins breaking down the muscle you just built for energy. Strength drops fast. Body fat creeps back.
Mood takes a serious hit. Low testosterone combined with oestrogen dominance produces symptoms that closely resemble clinical depression: low energy, no motivation, reduced libido, brain fog, and emotional instability. This is not weak mindset, it is a measurable hormonal state.
And it lasts longer than most people expect. A 2026 study from King’s College Hospital NHS Foundation Trust (published in BJU International, Ibis et al.) found that spontaneous hormonal recovery after steroid use takes 6 to 12 months without intervention. PCT was shown to significantly shorten that window, and the combination of hCG with clomiphene citrate produced superior recovery of both testosterone and semen parameters compared to SERMs alone.
Spontaneous recovery after steroid use takes 6–12 months without PCT. With the right protocol, that timeline can be cut to 4–8 weeks. Source: Ibis et al., BJU International, January 2026, King’s College Hospital NHS.
The Three PCT Drugs: Nolvadex, Clomid, and hCG
Every PCT protocol is built around one or more of these three compounds. Understanding what each one does, and where it fits, is the difference between a PCT that works and one that barely moves the needle.
| Nolvadex (Tamoxifen) | Clomid (Clomiphene) | hCG | |
|---|---|---|---|
| Drug class | SERM | SERM | LH analogue |
| How it works | Blocks oestrogen at pituitary → raises LH/FSH | Same mechanism, slightly weaker | Directly mimics LH, stimulates testes |
| Typical PCT dose | 20–40 mg/day | 50 mg/day (wks 1–2), 25 mg/day (wks 3–4) | 500–1000 IU every other day |
| Used alone? | Yes, for mild cycles | Yes, for mild/moderate | No, bridges to SERM use |
| Best suited for | Most cycles, solid default | Heavier suppression | Long/heavy cycles, testicular atrophy |
| Key side effect | Mild visual disturbances (rare) | Mood swings, hot flushes | Can cause desensitisation if overused |
Which One Do You Actually Need?
Mild cycle (Anavar, Primobolan, low-dose oral): Nolvadex alone at 20–40 mg/day for 4 weeks is sufficient for most users. It is the gentler SERM with fewer mood side effects.
Moderate cycle (single injectable, 8–12 weeks): Nolvadex or Clomid, either solo or combined at lower doses. 4 to 6 weeks is typically enough.
Heavy or long cycle (19-nor compounds, multiple injectables, 16+ weeks): Start with hCG to reactivate the testes before introducing SERMs. The 2026 King’s College data specifically highlighted hCG + clomiphene citrate as the superior protocol for recovery of semen parameters and testicular volume after aggressive cycles.
Clomid in particular is known to cause visual disturbances and mood instability at high doses. Many users now prefer Nolvadex as the default SERM precisely because the side effect profile is milder. Higher doses do not always mean better results.
When to Start PCT: Timing Guide by Compound
Starting PCT at the wrong time is one of the most common mistakes. Start too early and exogenous androgens are still clearing your system, making PCT largely ineffective. Start too late and you have already spent unnecessary weeks in a catabolic, low-testosterone state.
Timing is determined by the half-life of the last compound you used. Here is the practical guide:
| Compound Type | When to Start PCT | PCT Duration | Protocol |
|---|---|---|---|
| Oral steroids (Dbol, Anavar, Winstrol) | 24–48 hrs after last dose | 4–6 weeks | Nolvadex ± Clomid |
| Short-ester injectables (Test Prop, Mast Prop) | 3–5 days after last jab | 4–6 weeks | Nolvadex ± Clomid |
| Long-ester injectables (Test E, Test C, Deca) | 2–3 weeks after last jab | 6–8 weeks | hCG → then SERMs |
| SARMs (Ostarine, LGD, RAD-140) | 24 hrs after last dose | 4 weeks | Nolvadex or Clomid |
| Heavy stacks / 19-nor compounds (Tren, Deca) | 2–3 weeks after last jab | 8–12 weeks | hCG + Clomid + Nolvadex |
If you ran multiple compounds, time your PCT start based on the slowest-clearing drug in the stack, not the first one to clear. Deca Durabolin (nandrolone decanoate), for example, has a half-life of around 15 days. Starting PCT a week after your last Deca injection means you are still running on exogenous androgens.
How Long Should PCT Last?
PCT duration scales with cycle severity. A rough, practical framework:
- 4 weeks: Short oral-only cycles, mild SARMs, first cycles
- 6 weeks: Standard single or double injectable cycles, 10–14 weeks in length
- 8–12 weeks: Heavy stacks, long cycles, 19-nor compounds, or anyone who experienced notable testicular atrophy during the cycle
Blood tests are the only reliable way to confirm recovery. A morning testosterone measurement 4 weeks after PCT ends tells you whether your levels have returned to your personal baseline. If not, PCT extension and/or GP referral for endocrinology review is the appropriate step, not another cycle.
Do SARMs Need PCT?
Yes, depending on what you ran and for how long. The idea that SARMs are “suppression-free” is not accurate. As covered in our complete UK SARMs guide, all SARMs suppress the HPG axis to some degree. The question is severity.
Ostarine at low dose for 6–8 weeks: May recover without formal PCT. Monitoring with blood tests is still advisable.
LGD-4033, RAD-140, or YK-11, especially at higher doses or longer cycles: Suppression is meaningful and PCT is warranted. Nolvadex at 20 mg/day for 4 weeks is the standard starting point.
The same principle applies to SARMs as steroids: the stronger the compound, the higher the dose, the longer the cycle, the more robust the PCT needs to be.
What to Expect During PCT, Week by Week
PCT is not comfortable. Understanding what is normal stops people from panicking and abandoning the protocol midway.
Weeks 1–2: Energy is low, libido is minimal, mood is flat. This is the natural consequence of the hormonal crash that PCT is now addressing. Nolvadex or Clomid starts stimulating LH and FSH production, but testosterone levels have not climbed yet.
Weeks 3–4: Most people begin to notice small improvements in energy and mood. Libido starts to return. This is the SERM taking effect, LH and FSH are now rising and the testes are responding.
Week 5 onwards (for longer protocols): Testosterone continues climbing back toward baseline. Strength stabilises. The key at this stage is not to interpret improving symptoms as a green light to start another cycle. Give recovery the full time it needs.
Feeling better halfway through PCT does not mean your hormones have fully recovered. It means the process is working. Blood tests at the end of PCT, not how you feel, confirm recovery.
Training and Lifestyle During PCT
The drugs do the hormonal work. What you do every day determines how much muscle you keep.
- Train, but dial back intensity. Your recovery capacity is compromised. High-frequency, high-volume training is counterproductive when cortisol is elevated and testosterone is low. Train consistently but moderately.
- Eat at maintenance or a very slight surplus. A hard cut during PCT accelerates muscle loss. Prioritise protein at 1.8–2.2g per kg of bodyweight.
- Sleep is non-negotiable. The majority of testosterone secretion happens during deep sleep. 7 to 9 hours is the minimum for effective hormonal recovery, not a recommendation, a requirement.
- Manage alcohol intake. Alcohol suppresses LH secretion and raises oestrogen. Even moderate drinking during PCT meaningfully slows recovery.
- Consider: Zinc, vitamin D, and ashwagandha have modest but real evidence supporting testosterone recovery and cortisol management. They support PCT rather than replace it.
Signs Your PCT Is Not Working
If you are four to six weeks into PCT and experiencing the following, it is time for a GP consultation rather than waiting it out:
- Persistent severe fatigue with no improvement trend
- Zero libido or worsening erectile function after week 4
- Continuing gynaecomastia symptoms or nipple sensitivity
- Severe depression or mood instability beyond the early weeks
- Blood tests showing testosterone remains critically low at end of PCT
These signs may indicate anabolic steroid-induced hypogonadism (ASIH), a condition where the HPG axis does not restart properly. This requires endocrinology referral, not another SERM cycle. Your GP can arrange the appropriate tests and, if necessary, refer you to a specialist. Hormone replacement under medical supervision is a legitimate treatment for confirmed ASIH and is far safer than cycling further without recovery.
Frequently Asked Questions
What is the best PCT for a testosterone cycle?
Nolvadex (tamoxifen) at 20–40 mg per day for 4 to 6 weeks is the most widely used PCT for a standard testosterone cycle. If the cycle was long (16+ weeks) or involved testicular atrophy, adding hCG for 2 to 3 weeks before starting the SERM produces better recovery of testosterone and semen parameters, according to 2026 clinical data from King’s College Hospital NHS.
Do I need PCT after a SARMs cycle?
Most SARMs require some form of PCT. Compounds like LGD-4033 and RAD-140 cause meaningful testosterone suppression, and recovery without intervention can take months. Nolvadex at 20 mg per day for 4 weeks is a standard starting point. Low-dose, short Ostarine cycles sometimes recover without formal PCT, but blood tests are the only way to confirm this.
Can I use Nolvadex and Clomid together?
Yes, and this combination is used for heavier cycles. Nolvadex provides reliable oestrogen receptor blockade with a milder side effect profile; Clomid adds potent LH and FSH stimulation. Combined, they work on both sides of the hormonal recovery. However, both at full dose simultaneously increases side effect risk. Lower doses of each (Nolvadex 20 mg + Clomid 25 mg) are more commonly used than maxing out on either.
How do I know my PCT has worked?
The only reliable confirmation is a morning testosterone blood test taken 4 weeks after finishing PCT. Symptoms like returning libido and energy are useful indicators but not proof. If your testosterone has returned to your pre-cycle baseline, recovery is confirmed. If it remains significantly below baseline, speak to your GP about endocrinology referral.
Can I start another cycle straight after PCT?
The general guideline in bodybuilding communities is cycle length plus PCT length equals minimum time off before the next cycle. So a 12-week cycle followed by 6-week PCT means at least 18 weeks before starting again. Bloodwork confirming full hormonal recovery matters more than any timeline formula. Running consecutive cycles without confirmed recovery increases the risk of permanent hypogonadism.
Is PCT legal in the UK?
Nolvadex (tamoxifen) and Clomid (clomiphene) are prescription-only medicines in the UK. They are not controlled substances under the Misuse of Drugs Act, possession for personal use is not a criminal offence, but selling them without a licence is. hCG is also prescription-only. The MHRA advises against sourcing any prescription medicine from unregulated online suppliers due to dosing and contamination risks.
Disclaimer: This article is for educational and informational purposes only. It does not constitute medical advice. Nolvadex, Clomid, and hCG are prescription-only medicines in the UK. If you are experiencing symptoms of hormonal disruption after steroid use, consult a qualified GP or endocrinologist.