Testosterone replacement therapy is one of the fastest-growing areas of men’s health in the UK. Prescriptions have increased more than fivefold over the past decade, and private TRT clinics have proliferated across Britain to meet demand that the NHS, with its strict thresholds and long waiting lists, is simply not equipped to handle.
Whether you are experiencing the classic symptoms of low testosterone, fatigue, low libido, brain fog, loss of muscle mass, or you are a bodybuilder trying to understand how medical TRT differs from a steroid cycle, this guide covers the full picture. How diagnosis works, what your blood test numbers actually mean, NHS versus private treatment, every formulation available, the real benefits and risks, and exactly how to get started.
What Is TRT?
Testosterone replacement therapy (TRT) is a medically supervised treatment that restores testosterone to a healthy physiological range in men whose bodies are not producing enough of it. It treats a recognised medical condition called hypogonadism, a failure of the testes to produce adequate testosterone, caused by a problem either in the testes themselves (primary hypogonadism) or in the hormonal signalling from the brain (secondary hypogonadism).
TRT is not a performance-enhancing shortcut. It is the medical management of a hormonal deficiency, equivalent in principle to a thyroid patient taking levothyroxine or a diabetic taking insulin. The goal is to restore levels to the normal physiological range, not to push them into territory that generates supraphysiological anabolic effects.
That distinction matters particularly for the bodybuilding and performance community, where TRT is sometimes confused with steroid cycling. They share the same molecule, testosterone, but the dose, the intent, and the medical context are entirely different, as we address directly later in this guide.
Symptoms of Low Testosterone in Men
Low testosterone rarely announces itself dramatically. Most men experience a gradual decline in multiple areas over months or years before connecting the dots. The most commonly reported symptoms include:
- Persistent fatigue: not just tiredness, but a heavy, chronic low-energy state that does not resolve with sleep
- Reduced libido: a noticeable, sustained drop in sexual drive that is uncharacteristic for you
- Erectile dysfunction: difficulty achieving or maintaining erections, particularly in the morning
- Loss of muscle mass: declining strength and physique despite consistent training
- Increased body fat: particularly around the abdomen, even without dietary changes
- Mood changes: low mood, irritability, poor motivation, brain fog, or depression-like symptoms
- Poor sleep: difficulty falling asleep or waking frequently without explanation
- Reduced bone density: longer-term consequence; may only appear in scans
These symptoms individually can have many causes. Experiencing several simultaneously, particularly the combination of low energy, low libido, and body composition changes, is the clearest signal to get a blood test.
Low testosterone symptoms overlap significantly with depression, sleep disorders, and thyroid problems. A blood test is the only way to confirm whether testosterone is actually the issue. Do not self-diagnose based on symptoms alone.
How TRT Is Diagnosed in the UK
Diagnosis requires blood tests, specifically, at least two separate morning testosterone measurements taken before 11am, when testosterone levels are naturally at their peak. A single reading is not sufficient to diagnose hypogonadism because testosterone fluctuates day to day based on sleep, stress, and time of day.
What Your Blood Test Numbers Mean
Total testosterone is measured in nanomoles per litre (nmol/L) in UK labs. Here is the clinical reference guide for interpreting your results:
| Total Testosterone Level | What It Means | UK Clinical Response |
|---|---|---|
| Below 8 nmol/L | Clinically low (hypogonadism) | NHS will typically prescribe TRT |
| 8–10.4 nmol/L | Borderline low | NHS usually declines; private clinics may treat based on symptoms + free T |
| 10.4–12 nmol/L | Low-normal, grey zone | NHS rarely treats; private assess free testosterone, SHBG, and symptoms |
| 12–20 nmol/L | Normal range | TRT not indicated unless secondary symptoms suggest otherwise |
| 15–30 nmol/L | Optimal therapeutic range on TRT | Target range when on replacement therapy |
| Above 35 nmol/L | Supraphysiological, performance use | Not a TRT dose; anabolic territory; not medically prescribed |
Why Free Testosterone and SHBG Matter
Total testosterone is not the whole picture. Much of the testosterone in your blood is bound to sex hormone-binding globulin (SHBG) and is biologically inactive. Only free testosterone, the unbound fraction, is available to tissues and has an effect. A man with a total testosterone of 14 nmol/L and very high SHBG could have less biologically active testosterone than a man with a total of 10 nmol/L and low SHBG.
The NHS typically only measures total testosterone in initial assessments, which is one of the most common criticisms of the NHS TRT pathway. Private clinics routinely measure free testosterone, SHBG, oestradiol, LH, FSH, and prolactin, giving a far more complete hormonal picture.
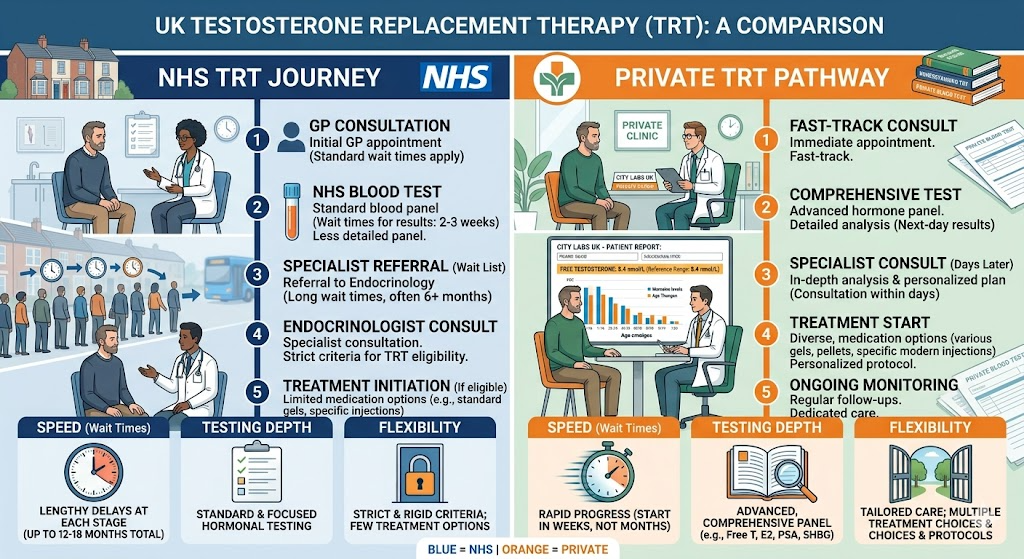
NHS TRT vs Private TRT in the UK: What’s the Difference?
This is where most men in the UK hit a wall. The NHS offers TRT, but accessing it is a more complex, slower, and less flexible process than most people expect.
| Factor | NHS TRT | Private TRT |
|---|---|---|
| Eligibility threshold | Below 8 nmol/L (strict) | More flexible, symptoms + free T considered |
| Speed of access | Weeks to months; GP first, then endo | Days to weeks; self-refer directly |
| Cost | £9.90/item NHS prescription charge | £99–£300+/month depending on clinic |
| Treatment options | Gels, long-acting injections (Nebido) | Injections (prop, enanthate, cypionate), gels, creams, pellets |
| Frequency of monitoring | Every 3–6 months if you can get an appointment | Every 3 months; included in most private plans |
| Blood tests included | Basic total T only in many cases | Comprehensive: free T, SHBG, oestradiol, haematocrit, PSA, lipids |
| Fertility support (hCG) | Not routinely offered | Available at most private clinics |
| Specialist TRT knowledge | GP or general endocrinologist | TRT-specialist doctors |
| Postcode lottery factor | Yes, significant variation by area | No, consistent UK-wide access |
The NHS Route
If your total testosterone is consistently below 8 nmol/L on two separate morning tests, your GP will typically refer you to an endocrinologist. The endocrinologist confirms the diagnosis, and TRT is prescribed. The whole process, from initial GP appointment to receiving treatment, can take several months to over a year, depending on area and NHS waiting lists.
A critical practical point: the NHS has a postcode lottery problem with TRT. Some areas have well-established men’s health pathways; others have minimal endocrinology resource, and GPs in those areas are reluctant to refer even clearly symptomatic men. NHS prescription cost is £9.90 per item, making it the most affordable option if you can access it.
The Private Route
Private TRT clinics across the UK have expanded rapidly since 2020 to meet demand from men who either cannot meet NHS eligibility thresholds or simply cannot wait. You do not need a GP referral to access private TRT, you can self-refer directly.
Private treatment typically begins within days of your first blood test. Costs in 2025 and 2026 range from £99 to £300 per month depending on the clinic, formulation, and what is included. Year one costs at a mid-range clinic run roughly £1,200 to £1,500 all-in, covering consultations, blood tests, medication, and injection supplies. Year two typically drops to £1,000 to £1,200 as diagnostic costs reduce.
The key advantage is clinical depth. Private TRT doctors measure free testosterone, SHBG, oestradiol, haematocrit, and PSA, and adjust protocols based on the full picture rather than a single number.
Types of TRT Available in the UK
Testosterone Injections
Testosterone enanthate and testosterone cypionate are the most commonly used injectable forms in private TRT. Injected every 7 to 14 days into the muscle or subcutaneously, they deliver stable blood levels with predictable results. Most TRT specialists consider injectable testosterone the gold standard for precise dose control.
Nebido (testosterone undecanoate) is a long-acting injectable available on the NHS, given every 10 to 14 weeks. It is convenient but less precise, levels can fluctuate significantly over the injection interval, and adjustments are slower to implement.
Testosterone Gels
Testogel and Tostran are topical gels applied daily to the shoulder, upper arm, or abdomen. They are widely available on the NHS and avoid injections, making them the most commonly NHS-prescribed form. The limitation is daily application, potential transfer to partners or children, and variable absorption rates between individuals.
Testosterone Patches and Creams
Patches are available but less commonly used in the UK due to skin irritation issues. Compounded testosterone creams are offered by some private clinics for more precise dosing than pre-manufactured gels allow.
What TRT Actually Does: The Realistic Benefits
TRT is not a transformation drug for healthy men with normal testosterone levels. For men with confirmed hypogonadism, the benefits are real, meaningful, and clinically documented. A 2025 patient survey by a leading UK private clinic found 90% of patients reported improvement in quality of life and wellbeing on TRT.
- Energy and vitality: Most men notice improvement in energy levels within 3 to 6 weeks. Fatigue that was persistent and debilitating typically resolves substantially.
- Libido and sexual function: Return of sexual interest is usually one of the first and most pronounced benefits, commonly reported within 3 to 4 weeks of reaching a therapeutic level.
- Mood and cognitive function: Brain fog lifts, motivation returns, irritability reduces. Men on TRT frequently describe feeling “like themselves again” after years of gradual decline.
- Muscle mass and body composition: Lean muscle is easier to build and maintain; body fat, particularly visceral abdominal fat, tends to reduce. These changes emerge over 3 to 6 months at therapeutic doses.
- Bone density: Long-term TRT reduces the risk of osteoporosis associated with hypogonadism. This is a slower benefit, measurable over 12 to 24 months.
- Cardiovascular markers: Emerging evidence suggests TRT in genuinely hypogonadal men improves insulin sensitivity, lipid profiles, and may reduce cardiovascular risk, though this requires appropriate dosing and monitoring.
These benefits only apply when testosterone was genuinely deficient to begin with. TRT does not provide anabolic enhancement above normal physiological levels, that is a different category of use entirely.
TRT Risks and Side Effects
TRT is safe when properly dosed and monitored. The risks below are real but manageable, and the reason regular blood monitoring is not optional, it is the entire safety framework.
Erythrocytosis (Elevated Haematocrit)
TRT stimulates red blood cell production. If haematocrit, the proportion of red cells in blood, rises too high (above 52–54%), blood becomes thicker and cardiovascular risk increases. This is the most clinically significant monitoring parameter on TRT. Regular full blood count tests detect it early, and dose adjustment or therapeutic venesection (blood donation) corrects it.
Testicular Atrophy and Fertility
TRT suppresses the HPG axis in the same way anabolic steroids do, your testes stop receiving LH and FSH signals and reduce in size and output. TRT typically makes you infertile while on it. This is reversible for most men after stopping, but recovery is not guaranteed, particularly after long-term use. Men who want to preserve fertility should discuss hCG (human chorionic gonadotropin) alongside TRT with their prescriber.
Oestrogen Elevation
Testosterone converts to oestradiol through the aromatase enzyme. On TRT, if oestrogen rises too high, symptoms include water retention, mood instability, and in some cases gynaecomastia. This is managed through dose adjustment or, in some cases, aromatase inhibitors, but crashing oestrogen with aggressive AI use causes more problems than mildly elevated oestrogen and should be avoided.
Acne, Oily Skin, Hair Loss
These androgenic effects are possible, particularly at higher doses or in men with genetic predisposition. They are more common in steroid use at supraphysiological doses than in properly managed TRT at physiological levels. Hair loss risk is relevant for men with a family history of male-pattern baldness.
Cardiovascular Considerations
Long-term TRT safety in the cardiovascular context requires monitoring. Recent large-scale studies, including the TRAVERSE trial, found no increase in major cardiovascular events in men on TRT compared to placebo, reassuring news, but still no reason to deprioritise the monitoring of blood pressure, lipids, and haematocrit throughout treatment.
TRT vs Steroids: What’s the Actual Difference?
This is one of the most commonly misunderstood distinctions in the fitness and men’s health space, including by some GPs who decline to prescribe TRT because they conflate it with performance steroid use.
Medical TRT restores testosterone to 15–30 nmol/L, the upper end of the normal physiological range. At this level, the body functions as it would with healthy natural production. Muscle gains are real but gradual; the primary benefits are hormonal balance, wellbeing, and health protection.
Anabolic steroid use pushes testosterone and related androgens to supraphysiological levels, commonly 2 to 10 times the top of the normal range. The anabolic effect is dramatically stronger, but so are the side effects: HPG axis suppression, cardiovascular strain, liver stress, and the hormonal crash that makes post cycle therapy essential.
The practical question for bodybuilders is: if you are on TRT, does it give you an edge in training? The honest answer is yes, relative to a hypogonadal man who is untreated. But properly managed TRT will not produce the body composition results of a steroid cycle. The molecule is the same; the dose is the variable that changes everything.
Some men use TRT as a “base” for performance cycles, maintaining a prescribed TRT dose year-round while adding anabolic compounds on top. This is not medical TRT. It is using a TRT prescription as cover for a steroid base. Prescribers are aware of this, and it carries the full risk profile of anabolic cycling.
How to Get TRT in the UK: Step by Step
Via the NHS
- Step 1: Book a GP appointment and describe your symptoms. Ask specifically for a testosterone blood test.
- Step 2: Get a morning blood test (before 11am). If results are borderline, request a repeat test and ask for LH, FSH, and SHBG to also be measured.
- Step 3: If total testosterone is below 8 nmol/L on two tests, your GP should refer you to endocrinology.
- Step 4: Endocrinology appointment. Specialist confirms diagnosis and prescribes TRT.
- Step 5: Collect prescription from GP or pharmacy. Pay standard prescription charge (£9.90/item).
Via a Private Clinic
- Step 1: Order an at-home finger-prick blood test or book a blood draw directly through the clinic.
- Step 2: Results reviewed by a TRT-specialist doctor. Comprehensive panel including free T, SHBG, oestradiol, PSA, and haematocrit.
- Step 3: Video or in-person consultation to discuss symptoms, results, medical history, and treatment options.
- Step 4: Prescription issued if eligible. Medication typically dispatched within days.
- Step 5: Monitoring blood tests at 3 months, 6 months, and annually thereafter. Dose adjusted as needed.
For context on how testosterone levels relate to what bodybuilders use, our guide on best testosterone booster supplements for UK men covers natural support options that can be used alongside or before committing to medical TRT.
Frequently Asked Questions
What testosterone level qualifies for TRT on the NHS?
The NHS typically prescribes TRT when total testosterone is consistently below 8 nmol/L on two separate morning blood tests. Men with levels between 8 and 12 nmol/L may qualify if there is a clear underlying cause. Private clinics apply more flexible criteria, assessing free testosterone, SHBG, and symptoms alongside total testosterone numbers.
How long does it take for TRT to work?
Most men notice libido improvements within 3 to 4 weeks. Energy and mood typically improve within 4 to 6 weeks of reaching a stable therapeutic dose. Body composition changes, more muscle, less fat, take 3 to 6 months to become clearly visible. Some men reach healthy testosterone levels within 6 weeks of starting treatment.
Does TRT make you infertile?
TRT suppresses sperm production by reducing FSH and LH signals to the testes, making most men infertile while on treatment. This is reversible for the majority after stopping, but recovery is not guaranteed, particularly after years of use. Men who want to maintain fertility should discuss adding hCG to their TRT protocol with their prescriber before starting treatment.
Can I get TRT on the NHS with symptoms but normal testosterone levels?
No. The NHS requires blood test confirmation of low testosterone (below 8 nmol/L) before prescribing TRT. Symptoms alone are not sufficient. If your levels are in the borderline range (8–12 nmol/L) and you are experiencing significant symptoms, a private clinic that measures free testosterone and SHBG may find a clinical basis for treatment that NHS testing missed.
Is TRT the same as taking steroids?
No. TRT restores testosterone to the normal physiological range (15–30 nmol/L). Anabolic steroid use pushes testosterone to supraphysiological levels, often 2 to 10 times higher than TRT doses. The molecule can be the same, but the dose, intent, and medical context are completely different. Properly managed TRT is a treatment for a hormonal deficiency, not a performance-enhancing drug.
How much does private TRT cost in the UK in 2025?
Private TRT costs range from £99 per month at budget-focused clinics to £200–£300 per month at full-service specialist providers. Year-one costs, including diagnostics and monitoring blood tests, typically run £1,200 to £1,800. Year two is lower as diagnostic costs reduce. NHS TRT costs only the standard prescription charge of £9.90 per item if you qualify and can access it.
Disclaimer: This article is for informational and educational purposes only. It does not constitute medical advice. TRT is a prescription-only medicine in the UK. If you are experiencing symptoms of low testosterone, consult your GP or a qualified healthcare professional before pursuing any treatment.


